Loneliness
Loneliness
Mental Health
Depression
Elderly Care
Older People
Healthy Ageing
Young People
Quality of Life
Five Ways to Wellbeing
Healthy People
Personal Wellbeing

 Introduction
Introduction
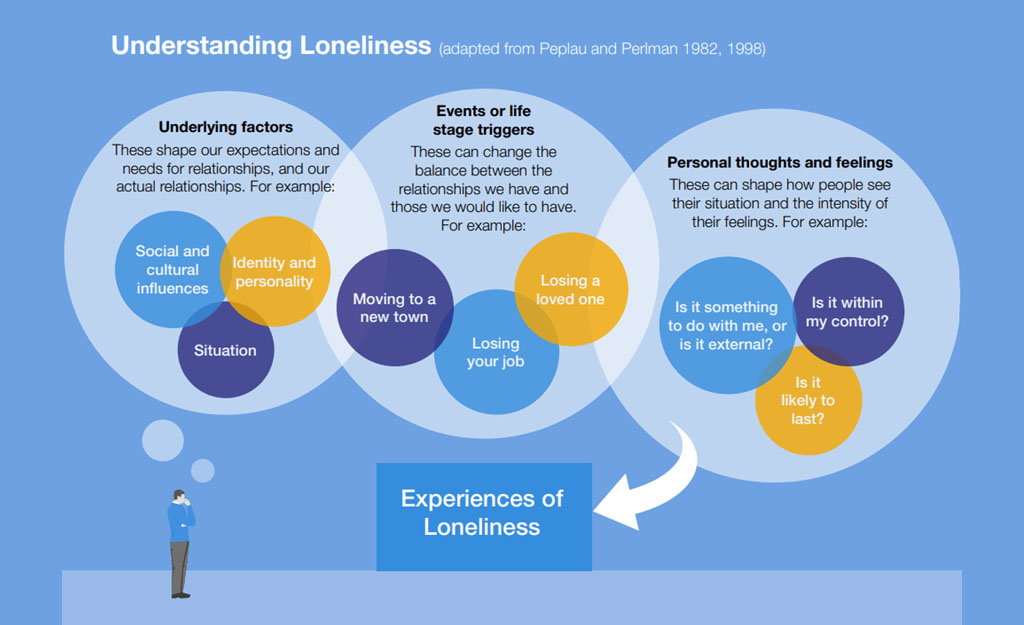
Loneliness is a uniquely personal experience that is often described as ‘a subjective, unwelcome feeling of lack or loss of companionship. It happens when we have a mismatch between the quantity and quality of social relationships that we have, and those we want’.1,2 Loneliness does not always correlate with being alone, the saying “have you ever felt lonely in a crowded room” goes someway to describing this. Loneliness can come and go at different times in our life and can be situational, for example only occurring during particular times of the year.
Although they often occur together, social isolation is distinct from loneliness in that it refers to someone being isolated from their community due to a range of external factors.3 These might be having fewer people to interact with socially due to lack or limited transport, financial, health conditions or isolated living conditions such as in rural areas.
Source DDCMS Loneliness Strategy
Anyone can experience loneliness, however, there are some groups who are more likely to experience and report loneliness than others. For example, older adults,4 people with a disability or poor physical or mental health,5 people who live alone or work shifts, carers (particularly unpaid),6 individuals from the LGBTQ+ community or people with neurodiversity.7 There are shared experiences within these population groups that may impact on their experience of loneliness such as lack of likeminded social network, reduction in good public transport and local activity, inability to maintain consistent employment, or connection with others. A key issue identified as impacting further on loneliness is also stigma associated with stereotypes about the type of people who may be lonely or lack of social connection which makes those experiencing it less likely to ask for help.8 In particular, when we think of loneliness we often think of older adults. Whilst research indicates older adults do experience higher than average levels of loneliness the impact of loneliness on the wide range of individuals identified in this key topic summary is important to consider, particularly when thinking about the impact on a persons long term health equity.
 Why is it important to Population Health?
Why is it important to Population Health?
Loneliness is vital to understand from a population health perspective due to not only the direct indications of loneliness on health and wellbeing but it’s link with other conditions which further impact an individual’s health.
Loneliness increases the likelihood of premature mortality by 26% and we know that feeling connected to other people helps you stay well, both physically and emotionally.9 We also know that having good quality social connection helps improve resilience both for individuals and for wider communities.10

Adapted from Health matters: Community-centred approaches for health and wellbeing - GOV.UK
When thinking of our population and why loneliness has such an impact, we can consider that if people are struggling with loneliness and social isolation, they are less likely to reach out for either physical or emotional support or guidance resulting in worsening health when they do seek help. People who are lonely are also less likely to engage with positive health behaviours such as reducing smoking, eating healthily, taking medication as prescribed.11
Poor mental health can also lead to loneliness as people tend to withdraw from existing social connections and support services, therefore further confounding their perceived loneliness or lack of support. There is also a link with older adults, dementia and loneliness due to reduction in cognitive ability to process their experience.12
These outcomes not only impact on individual’s health and wellbeing, they also bring systemic pressures to the health and social care system in terms of increased demand and/or increased complexity as people’s ability to reach out for early, preventative support reduces.13
 The Derbyshire Population Health Approach
The Derbyshire Population Health Approach
The Derbyshire Population Health Approach focuses on prevention, population health, evidence-informed practices, causes, and collaboration. It emphasises proactive measures to prevent health issues, tailors interventions to specific populations, incorporates evidence-informed practices, addresses underlying causes, and promotes collaboration for effective action.
When considering the topic of loneliness within The Derbyshire Population Health Approach:
• Prevention
From a strategy perspective, enabling resilient, thriving and connected communities is a priority for Joined Up Care Derbyshire ICB, Derbyshire County Council Public Health and Adult Social Care, among other statutory partners, as part of work to prevent or delay social care & health needs in the population.14,15 Community & Voluntary sector infrastructure organisations and community providers are vital partners in this preventative work, both on a micro level via working with individuals experiencing social isolation and loneliness, and a system level through informing and providing evidence to inform strategy development and commissioning. The county wide Health and Wellbeing Team also promote social interaction through facilitating connection with community based initiatives.
In Derbyshire there are a range of preventative schemes and initiatives that have an intended outcome of preventing loneliness and improving social connection, these include time swapping and volunteering, peer support groups, social prescribing, digital inclusion, locality partnerships offering micro grants for schemes such ‘social connectedness’ and stakeholder engagement forums.
Until recently much of the preventative focus around loneliness in Derbyshire has been aimed at older adults, including unpaid carers and those living in rural areas – with commissioned providers such as Age Uk and Derbyshire Carers Association tasked with finding ‘hard to reach’ pensioners and carers to provide a range of support including improving wellbeing via increased social connection. However over recent years national studies show that younger cohorts, such as single females and renters, are found to have increased risk of social isolation. Raising awareness of this, including busting myths about loneliness generally, is a priority for Public Health as part of preventative work.
A key campaign that underpins preventative strategy in Derbyshire related to social isolation is the 5 Ways to Wellbeing (connect, be active, take notice, keeping learning, give back) and this simple and effective framework16 is used and promoted by a variety of partners to help deliver messaging to providers and the public about the importance of social connection and other factors on wider health and wellbeing outcomes.17
• Population
- There are various demographic groups in Derbyshire who are more likely to experience loneliness and social isolation pointing to inequalities. These include more obvious groups such as older adults, unpaid carers, those with disabilities/health conditions and those living in rural areas.
- Derbyshire has a higher percentage of the population who are aged 65+, unpaid carers and those living in rural areas than the England average. Older adults aged 50+ are 3.7 times more likely to be often lonely if they are in poor health.18 In addition, fewer unpaid carers in Derbyshire report having as much social contact as they would like – 19.3% of adult carers in Derbyshire compared to 22.6% in England – indicating that there is particular social impact on carers in Derbyshire related to isolation.
- There are less obvious groups who studies show are more at risk of isolation, including single working age adults (especially females), those who rent a property (due to unstable tenancies and frequent moving), those experiencing domestic violence and single parents on low incomes. South Derbyshire has seen a significant increase in working age people in recent years, as people move into the area for work and to find housing in the district’s growing urban areas.
- As part of Public Health’s Digital Inclusion Strategy 2023–2026, a phone poll revealed 20% of adults in Derbyshire did not use the internet or needed help to use it – with 9% not using the internet at all. 14.1% of Derbyshire adults do not have access to a smartphone19
- Younger people are also increasingly affected by loneliness, with young carers and care leavers key groups more likely to face isolation and other increased risked factors for poor wellbeing.20 A key finding of the 2024 My Life, My View survey was that poor emotional wellbeing is associated with increased health-risky behaviour.
- In addition, young people are increasingly communicating online which can lead to the positive of more diverse and wide reaching social groups. The 2024 My Life, My Way survey found 92% of pupils said they were glad they can use devices to talk to friends when they can’t meet up – agree or strongly agree – but online communication can also lead to loneliness if someone is being bullied online or struggling with self-image.
- The 2024 My Life, My View survey found that out of six categories, ‘the way they look’ was the most common worry young people faced (45%), with ‘relationships with friends’ being 3rd at 33%. In addition, 35% of boys and 52% of girls had often or always felt either sad, angry, depressed, hopeless or lonely in the past two weeks.21
- Those living in lower income households are more likely to experience social isolation. 15% of children in Derbyshire live in deprived households as of 2019. The Good Childhood Index survey found that 27.5% of children who received free school meals reported they are often lonely, compared to 5.5% of those who do not. In Derbyshire around 31,000 children are eligible for free school

Studies show that loneliness can increase the risk of early mortality by 26%.22 However, loneliness can be difficult to detect or recognise as those who are isolated are less likely to be known to services until the issue is acute and/or is negatively affecting health and wellbeing to the point that help from services is required. This can be due to lack of awareness in the population and self-stigmatising of those experiencing loneliness.
Almost everyone knows that smoking or obesity is bad for health and can lead to early death, but the comparable effect of loneliness and isolation upon health is not well known by the general public. Campaigns such as the Campaign to End Loneliness and many of Age UK’s campaigns do important work to raise awareness and suggest solutions and mitigations.23
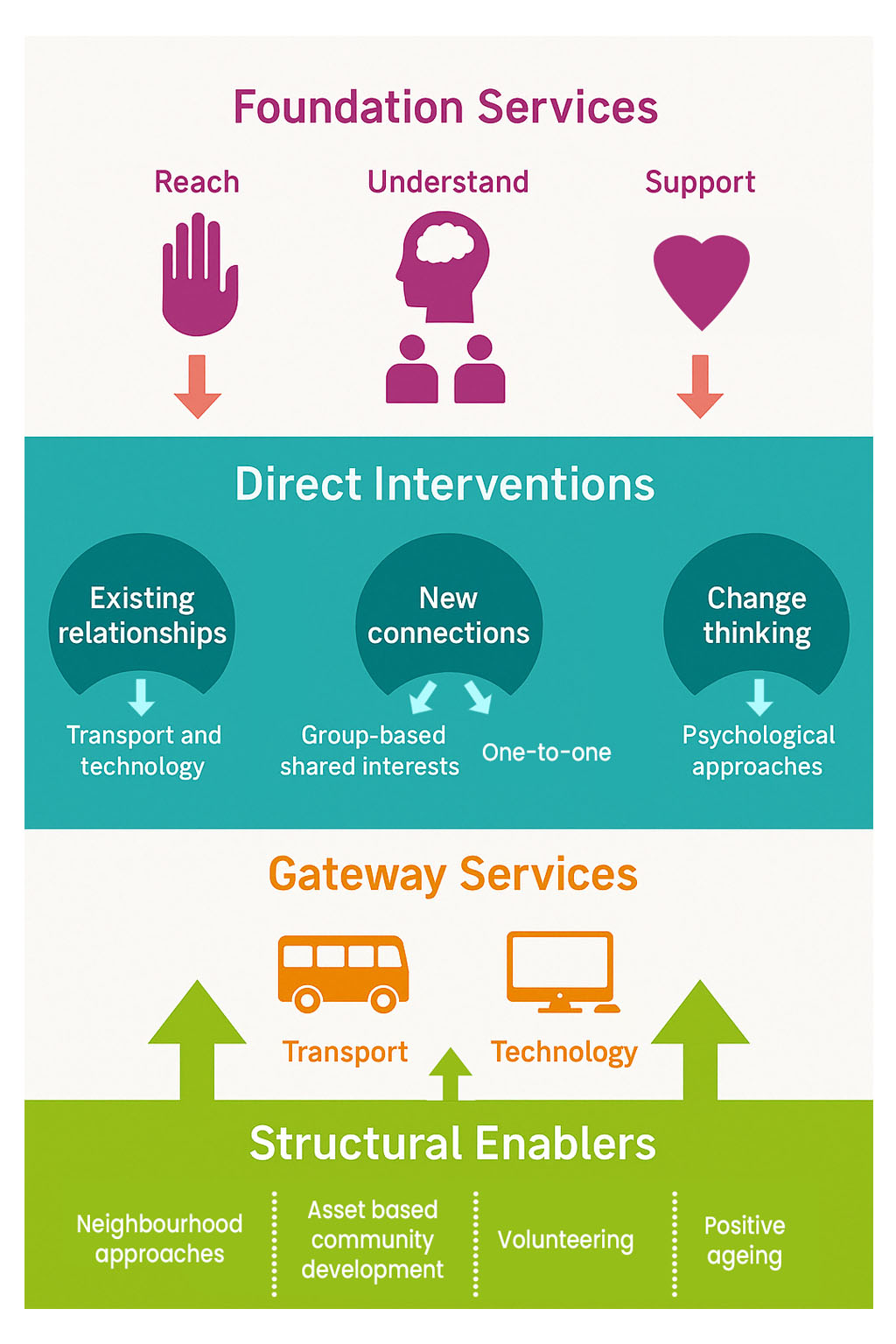
Age UK’s recent ‘Loneliness in Later Life 2024’24 report looks at ways to address loneliness finding that a range of solutions is required and that no ‘one size fits all’. This mirrors the conclusions of DCMS25 who evaluated interventions to tackle loneliness. These reports and others found that a ‘whole system’ approach is required, that includes ongoing education/awareness raising campaigns for the public and professionals (Understand), a system of direct interventions for a range of cohorts at differing levels (Reach) and a psychological approach providing help such as peer support, talking therapies, bereavement counselling and CBT (Support).
Adapted from Campaign to End Loneliness
• Causes
Derbyshire has a number of rural areas, particularly in the Derbyshire Dales and High Peak areas. Evidence shows living in a rural area can be a key environmental cause of loneliness and isolation, particularly in older people, as people living in rural areas may experience poor transport links and have less digital access. Local Community and Voluntary organisations in Derbyshire play a vital role in these and other communities, working on the ground to identify and support ‘hard to reach’ residents and help them access support and opportunities to reduce loneliness.
The causes of isolation can be physical – such as social isolation due to limited mobility or unpaid caring duties meaning a person is unable to get out and about to socialise and connect with people.26 For younger people moving away from family and friends for work or to find suitable housing can lead to isolation, as can modern trends of working from home.27 Financial deprivation can also cause or increase loneliness as lack of resources impact on the ability to socialise, travel, enjoy experiences with friends and even keep in touch online.28
Loneliness and social isolation can also be exacerbated by mental ill health or stigma and get worse over time as a person increasingly withdraws from society as their anxiety or level of depression increases. This is a significant risk as those who are socially isolated are less likely to seek medical help, reducing the opportunity for earlier intervention.
Social isolation can creep up on people gradually over time as social connections fade as people’s lives change. In other cases, unexpected situational causes such as a relationship break up, bereavement or children/family moving out of the area can cause people to feel loneliness all of a sudden and become overwhelming.
In an increasingly online world digital exclusion can also lead to or increase loneliness as those without the skills/access struggle to keep in touch with friends and family.
• Collaboration
In Derbyshire the impact of loneliness and social isolation on wider health and wellbeing outcomes, and its impact on early deaths/healthy life expectancy, is well recognised by Health, Social Care and other system partners working at county wide, locality and community level. Recent Council budget pressures has meant that focus has had to be directed to statutory and acute services, but this is not a reflection of the value placed on preventative support or services that enable social connection and wellbeing.
The 2024-2027 Public Health Strategic Plan29 has focus area of ‘protecting and enabling people of all ages to live safe and healthy lives’. This includes supporting people to maintain good health, minimise ill health and prevention of early deaths. Reducing social isolation and improving wellbeing are seen as key enablers of this priority with a commitment to work closely with ICS partners to reduce health outcome inequalities. Similar strategic aims and language are featured in the strategic plans of Derbyshire County Council, Joined Up Care Derbyshire and other local organisations
Work to collaborate on social isolation and loneliness is well driven by local health and wellbeing partnerships which include professionals from local authorities, health, housing, other statutory sector organisations, community and voluntary sector organisations and others. This includes the commissioning / micro-commissioning of services, schemes and activities with outcomes including social and emotional wellbeing. The benefit of localities work is the ability for collaborators to focus in on local need – identifying groups or cohorts most at risk and working to address inequalities as much as possible.
Public Health and partners place value on developing community resilience through enabling members of communities to provide support to each other, whether practical or emotional. There are various teams and services, both in-house and commissioned, who work to link community members together in various ways, formal and informal. Examples include reciprocal schemes such as Time Swap, offering micro-grants and support for people to set up and run activities in their communities and linking people up through buddying and peer support groups. This work sees a wide range of services and professionals working together and sharing contacts to build networks.
 Latest Derbyshire Data
Latest Derbyshire Data
Derbyshire Quilt
Prevalence Maps of Derbyshire
The maps below illustrate Lower Super Output Areas (LSOAs) and Middle Super Output Areas (MSOAs) for Derbyshire. LSOAs and MSOAs are geographical divisions used for statistical purposes, allowing for more detailed analysis of local data. In these maps, you can explore various health indicators and data for Derbyshire, providing valuable insights into the area’s health and wellbeing.
 |
In the top right of the map, you’ll find the ‘Layer Control’ icon. This is an easy way to customise what you see on the map visualisation. Click the ‘Layer Control’ to choose which information is displayed on the map. Pick the indicator that interests you the most, and the map will transform accordingly. |
Slope Index
This chart illustrates the differences in health and lifestyle factors across areas in Derbyshire, from the most deprived (decile 1, red) to the least deprived (decile 10, green). As you move from left to right on the chart (from more deprived to less deprived areas), the line shows whether these factors are becoming more or less common. Essentially, it’s a way to see how living in wealthier or poorer areas affects the prevalence of these factors.
 Further Analysis & Assessments
Further Analysis & Assessments
Derbyshire Joint Strategic Needs Assessment (JSNA) involves a thorough examination of a specific health problem, exploring its causes, consequences, and underlying factors. It combines various data sources, collaboration with stakeholders, and rigorous analysis to generate insights for evidence-informed interventions and policy changes.
 More Information & Resources
More Information & Resources
Here is a list of useful resources and information with regard to loneliness. These materials are meant to provide individuals, healthcare professionals, and communities with the knowledge and tools they need as part of efforts to address loneliness as a population health topic.
Contributors
Jay Patient, Public Health Lead, Community Support & Resilience
Alex Shore, Public Health Service Manager, Community Support
Jess Wilson, Public Health Group Manager, People and Place
Aariana Sohal, Health and Wellbeing Coach, Health and Wellbeing Team
Footnotes
Perlman & Peplau (1981) Toward a social psychology of loneliness↩︎
A Connected Society: A strategy for tackling loneliness - laying the foundations for change | HM Government↩︎
Social Isolation and Loneliness | World Health Organisation↩︎
Poll reveals extent of loneliness for Disabled people | Disability Rights UK↩︎
10 facts about loneliness and caring in the UK for Loneliness Awareness Week | Carers UK↩︎
Loneliness Stigma Rapid Evidence Assessment (REA) | gov.uk↩︎
Community Life Survey 2021/22: Wellbeing and loneliness | gov.uk↩︎
The Community Paradigm: Why public services need radical change and how it can be achieved↩︎
Social Engagement and Brain Health | Global Council on Brain Health↩︎
Economic gradients in loneliness, social isolation and social support: Evidence from the UK Biobank↩︎
Building people’s resilience and social connections | Think Local Act Personal↩︎
Derbyshire Public Health’s Digital Inclusion Strategy 2023-2026↩︎
Loneliness and social isolation as risk factors for mortality: a meta-analytic review (2015)↩︎
Promising approaches to reducing loneliness and isolation in later life | Campaign to End Loneliness & Age UK↩︎
You are not alone in feeling lonely: Loneliness in later life | Age UK↩︎
Children’s and young people’s experiences of loneliness: 2018↩︎
Investigating factors associated with loneliness in adults in England | gov.uk↩︎
Public Health Strategic Plan 2024-2027 | Derbyshire County Council↩︎